Cataract Surgery
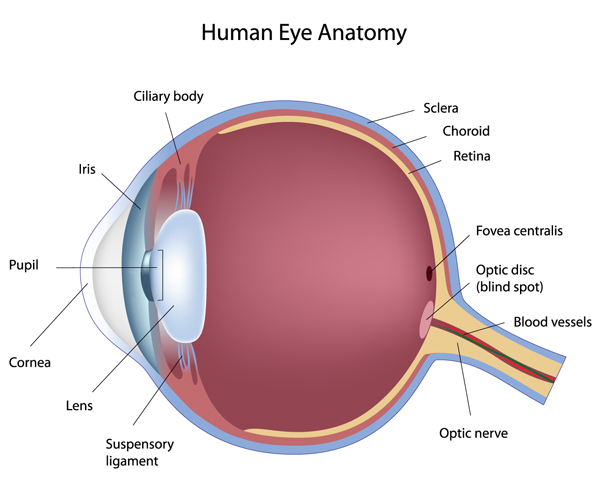
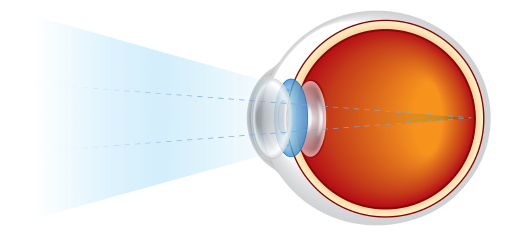
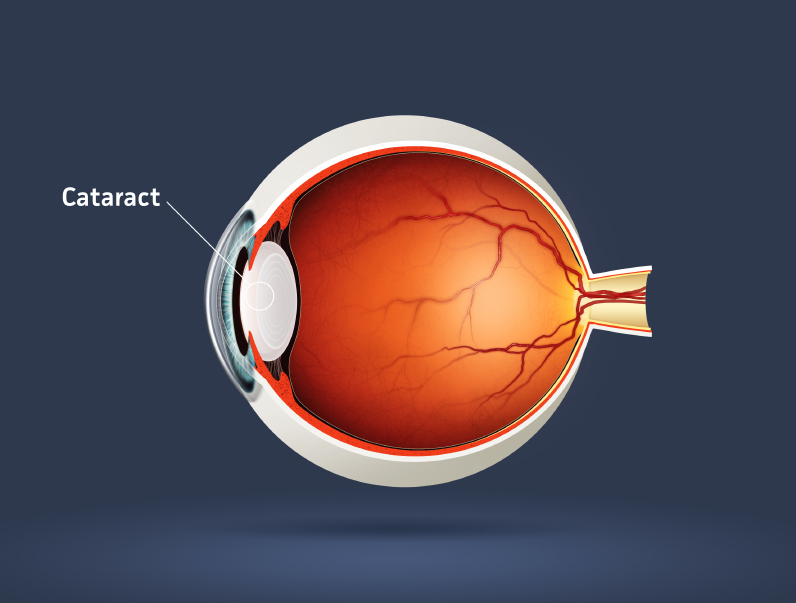
What is a cataract?
Do I need to have cataract surgery?
How long does the surgery take and what kind of aneasthetic will I have?
Mr Kashani tends to perform majority of his cases under topical aneasthesia. This type of aneasthetic uses strong drops to ‘numb’ the eye and it works very well. Of course for those whom are of a nervous disposition, other types of aneasthesia including subtenons (injection around the eyeball), sedation or general aneasthsia can also be employed. The main advantage of using topical aneasthesia is faster recovery post operatively with minimal discomfort to the patient. Mr Kashani will discuss provide a list of precautions after surgery with a number to call in case of any questions.
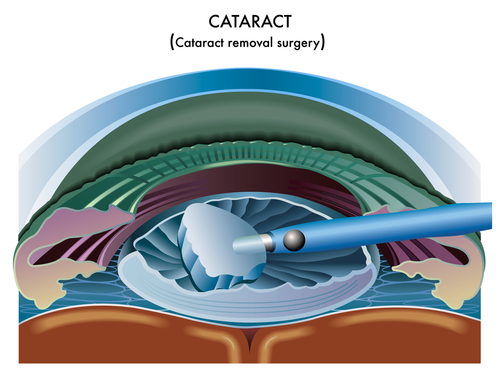
What happens during cataract surgery?
Will I get a cataract again?
How long will I need off work and how quickly will my eye take to heal?
Am I going to be admitted to hospital overnight?
What are the risks?
When can I drive?
Will I need glasses afterwards?
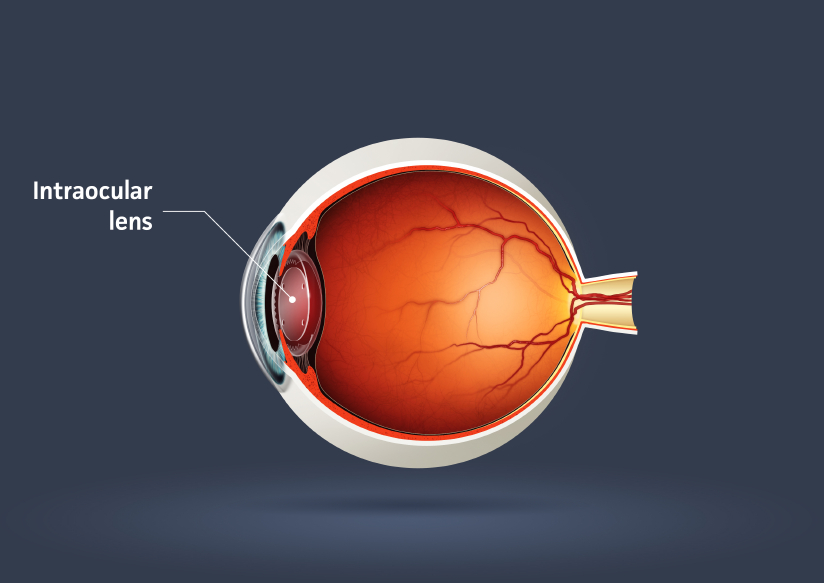
However ‘premium lenses’ exist (e.g toric, multifocal) which can correct both near and far vision as well as astigmatism, reflecting the function of the natural lens. Patient selection and discussing patient expectations is of paramount importance when choosing a premium intraocular lens. At the time of your consultation, Mr Kashani will go through the list of pros and cons of having a premium intraocular lens in comparison to a monofocal intraocular lens and he will discuss what you may expect after the surgery. It is important to choose the correct lens as ‘lens exchange’ requires further surgery and should be avoided if possible due to surgical risk.
What if I have other co-existing eye conditions?
What are the advantages of having the surgery privately?
Some clinical commissioning groups (CCG’s) are now placing in thresholds for first and second eye surgery in NHS in order to provide and prioritize the surgery to those who need treatment the most. Although almost all patients with visually significant cataract should still qualify, there will be some who sadly won’t and will have to wait until the vision worsens.
Finally the option of a “premium lens” in order to achieve spectacle independence following cataract surgery is only available on a private basis.
